Leg Length Discrepancy and Short Right Leg Syndrome
in the context of Remedial Therapy
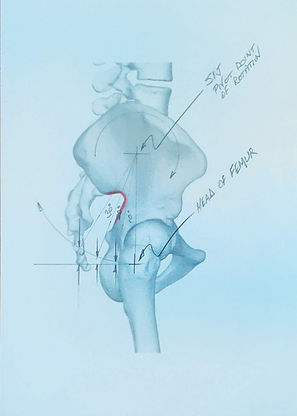
First Cardinal Sign, Assessment of Hip Posture – Standing and Prone
Anterior rotation of the hip in the Sagittal plane about the sacro-iliac joint on the side of the longer leg is an unconscious anatomical adjustment functionally pulling up the structurally longer leg and reducing pelvic tilt in the Frontal Plane. Giving the spine some protection and making us feel more comfortable standing. I rate the degree of rotation from Level successively through to Very High Range.
Cases presenting with the left hip in High Range anterior rotation is so common I call it normal. The literature describes range of motion at the SIJ limited to 4 degrees in any direction. It may be that the 30 degrees sighted across the hip in the standing position in part includes movement of the sacrum as well. However, this does not necessarily account for the 26 degrees beyond normal range of motion because I remind you the right hip/ilium is typically still level.
Measuring the difference in height between the top corner of the ASIS and the Iliac Crest as follows:
a. Low Range, 10mm or less (0 to 5 degrees);
b. Medium Range, 20 - 40mm (10 to 15 degrees);
c. High Range, 50 - 60mm (20 to 30 degrees); and
d. Very High Range, greater than 60mm...the largest sighted being approximately 100mm (45 degrees).
In actual practice I estimate the degree of rotation by eye without the use of tape measure or protractor. I have had extensive experience measuring, cutting and assembling things since the age of 10, including professional construction experience. Making fine judgement of distance and alignment is a learned skill not gained in university study. You do not give the apprentice the task of making critical measurements. While smaller intermediate angles might be hard to judge by eye but if you are seeing a 30 or 45 degrees angle, this is easily sighted, you know it is high range and many times beyond the normal range of motion for the SIJ described in the literature.
Level to Low Range is the ideal hip alignment in the upright standing position. This might be considered normal or good posture but it is not the norm. In my clinical experience, the majority of clients present with chronic left sided unilateral anterior hip rotation in High Range and a level right hip.
There are exception cases who have a structural leg length discrepancy and do not exhibit the First Cardinal Sign. This is uncommon. Pelvic tilt in the Frontal Plane will be greater and symptomatically they are more affected in the lumbar spine. Do not assume leg length is even or near even if the First Cardinal Sign of anterior rotation of the left hip is not present. Complete the examination for the other Cardinal Signs and structural leg length discrepancy tests before making conclusions.
I carry out an assessment of this aspect of hip posture following initial discussion of the client’s condition prior to treatment. Practitioner seated to the side of the client standing looking straight ahead. Noting Lordosis, Kyphosis, forward head carriage, and degree of chest tightness. Hip orientation in the Sagittal Plane is examined by palpating the Iliac Crest and top corner of the ASIS to determine hip position on both left and right sides.
My preference is to do the standing assessment, however, it is also possible to do so with subject lying prone. In the standing assessment we are looking at the hip position in relation to a horizontal line parallel to the floor. In the prone position it is in relation to a vertical line perpendicular to the floor. I have some concern gravity force vectors rotated 90 degrees from the standing position may distort test results. I have not made a close study comparing the test in different positions, yet it does seem to give a similar indication of hip alignment. I resort to testing in the prone position when reacquainting myself with a particular client’s condition or checking for progress during the course of a treatment. It is a quick, non-invasive although sometimes ticklish test to carry out.
I disagree with reports stating the prone position forces the rotated hip back into a neutral position. This occurs in supine, not prone. When lying on the back, weight of the body pushing up through the left glutes pushes the rotated left hip back toward the neutral position. Hence, why assessing relative ASIS heights in the Frontal plane standing is markedly different to supine on the treatment table. In standing the left hip is typically elevated 3mm to 5mm over the right. Unless they are an exception case where the First Cardinal Sign is absent. In which case, the left ASIS will be closer to 10mm higher. When in supine on the table this will change and an increase of up to 20mm or more will be will be observed. This is still only an indicator which ususally is close to actual discrepancy but it is not a direct measurement of leg length discrepancy owing to the vagaries of hip alignment.
Testing hip posture in the prone position, place the thumb on the Iliac Crest and forefinger on the top corner of the ASIS. Visually sighting the height difference front to back is not really possible. It becomes a judgment made by feel and estimating the distance off vertical. Comparison to the opposite side which you may have previously tested and know to be level aids judgement. If you are not confident with your ability to make this assessment in the prone position, refrain from doing so and rely on the standing assessment.
Testing hip flexor tightness is helpful assessing the First Cardinal Sign. The left hip being held in chronic anterior rotation shortens hip flexors (Iliacus in particular) and they will be tighter than the right hip flexors. This can be done by direct palpation or with the Thomas Test. Morphing the Thomas Test into a hip flexor stretch on the left side can be the quickest way to partially normalise hip position and alleviate acute symptoms in the backline of the left lower limb. I normally use a PNF stretch technique to do so.